
Medicare Part D plans significantly increased restrictions on prescription drugs, excluding more compounds from coverage or subjecting more of them to review before patients could access the treatments, according to a new study from USC researchers.
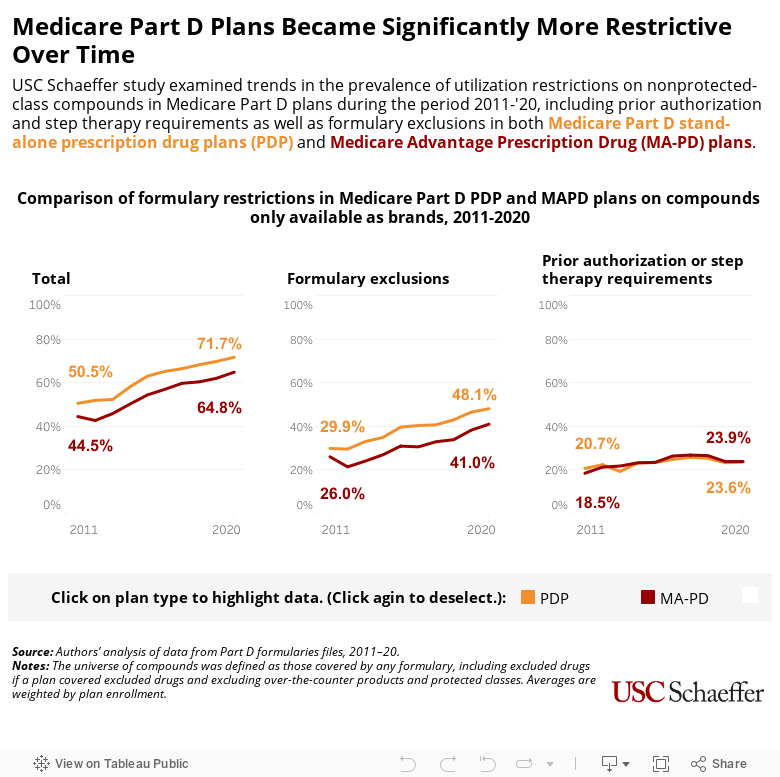
Among drugs not in Medicare “protected classes,” the share of drug compounds restricted or excluded by Part D plans surged from an average of 31.9% in 2011 to 44.4% in 2020, according to the study published in Health Affairs. Brand-name-only compounds (those without a generic alternative) were especially limited, with more than two-thirds of them subject to utilization restrictions or excluded from coverage altogether, researchers found.
Provided through private insurance plans that contract with the government, Medicare Part D is a prescription drug benefit for people with Medicare. In 2023, more than 50 million of the 65 million people covered by Medicare were enrolled in Part D plans, according to KFF.
Pharmacy benefit managers and health plans argue that such restrictions help control costs by ensuring patients do not use more expensive treatments when less expensive but equally effective therapies are available. But the large and increasing number of compounds that are subject to review or excluded from coverage raises concerns of the impact on patient health, researchers say.
“There are a lot of drug classes that are heterogeneous, where one drug may work for one patient but another drug may work for a different patient, so there are cases where this could be detrimental,” said study lead author Geoffrey Joyce, director of Health Policy at the USC Schaeffer Center for Health Policy & Economics. “This could lead to negative outcomes for patients that are not being considered.”
Using Medicare data, researchers examined trends in Part D plans excluding compounds from coverage or applying one of two utilization restrictions: “prior authorization,” which require plan members to get approval before filing a prescription; or “step therapy,” which require plan members to try a different medication before using the prescribed one.
Researchers conducted their analysis at the drug compound level. A drug “compound” includes branded and generic versions of a drug when they exist, and does not distinguish between them. Compounds were classified as “brand-name only” if no generic version existed in that year. All other compounds were classified as “generic available.”
The study found:
- In 2011, plans excluded, on average, 20.4% of compounds and subjected another 11.5% to prior authorization or step-therapy restrictions. By 2020, plans excluded 30.4% of compounds and placed another 14% under prior authorization or step therapy.
- Restrictions were more common among brand-name-only compounds, among more expensive compounds, and in stand-alone prescription drug plans compared with Medicare Advantage prescription drug plans.
- By 2020, 3 in 10 generic-available compounds and more than two-thirds of brand-name-only compounds in unprotected classes were restricted or excluded from coverage altogether.
Study co-author Karen Van Nuys, executive director of the Value of Life Sciences Innovation at the Schaeffer Center, noted that the rise in restrictions and formulary exclusions occurred as premiums for plans increased.
“Plans are charging more and they’re covering less, so it’s a double whammy,” Van Nuys said.
The increasing reliance on formulary exclusions was especially striking, researchers said. In the past, a patient wanting a certain drug might face a higher co-pay, noted Joyce, chair of the Department of Pharmaceutical and Health Economics at the USC Alfred E. Mann School of Pharmacy and Pharmaceutical Sciences. With plans now refusing to cover many drugs at all, only patients who can afford to pay the full price out of pocket can get that medication.
“For expensive drugs, that basically takes that treatment off the table,” Joyce said.
About the study
This research was supported by grants from the American Medical Association and the National Institute on Aging, National Institutes of Health (Award No. R01-AG055401). In addition to Joyce and Van Nuys, the study was co-authored by Barbara Blaylock, founder of Blaylock Health Economics LLC, and Jiafan Chen, a PhD student at USC.